Heart disease is rising rapidly in India, and Kolkata has become a major hub for advanced cardiology treatments. Among the leading specialists, Dr. Avishek Saha has earned a strong reputation for providing cutting-edge heart care, minimally invasive treatments, and compassionate patient support.
In this blog, we explore why more families in Kolkata are choosing Dr. Saha for their cardiac care and how his expertise is helping patients avoid major surgeries, recover faster, and live healthier lives.
❤️ 1. Expertise in Minimally Invasive Heart Treatments
Unlike traditional open-heart surgery, minimally invasive cardiology offers:
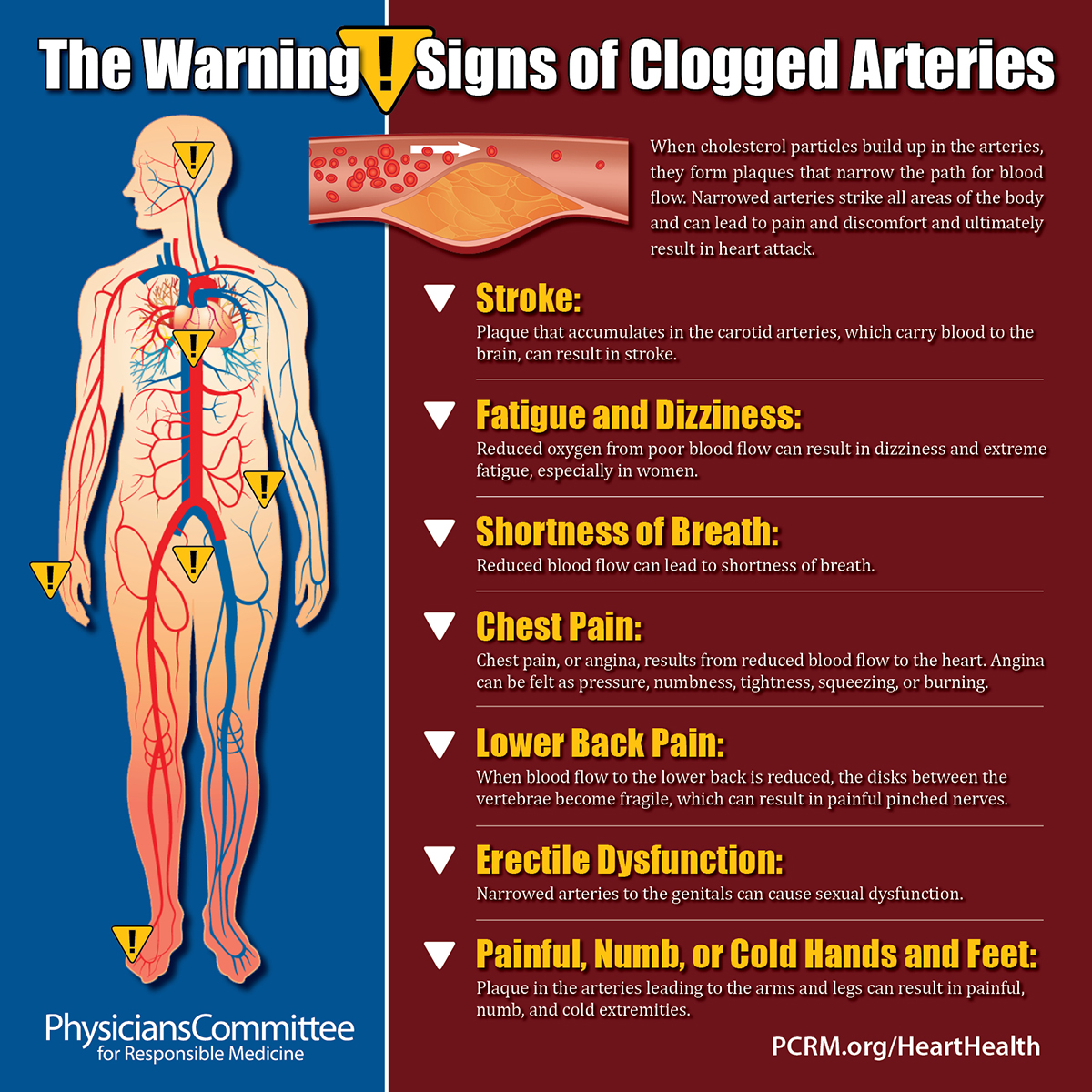
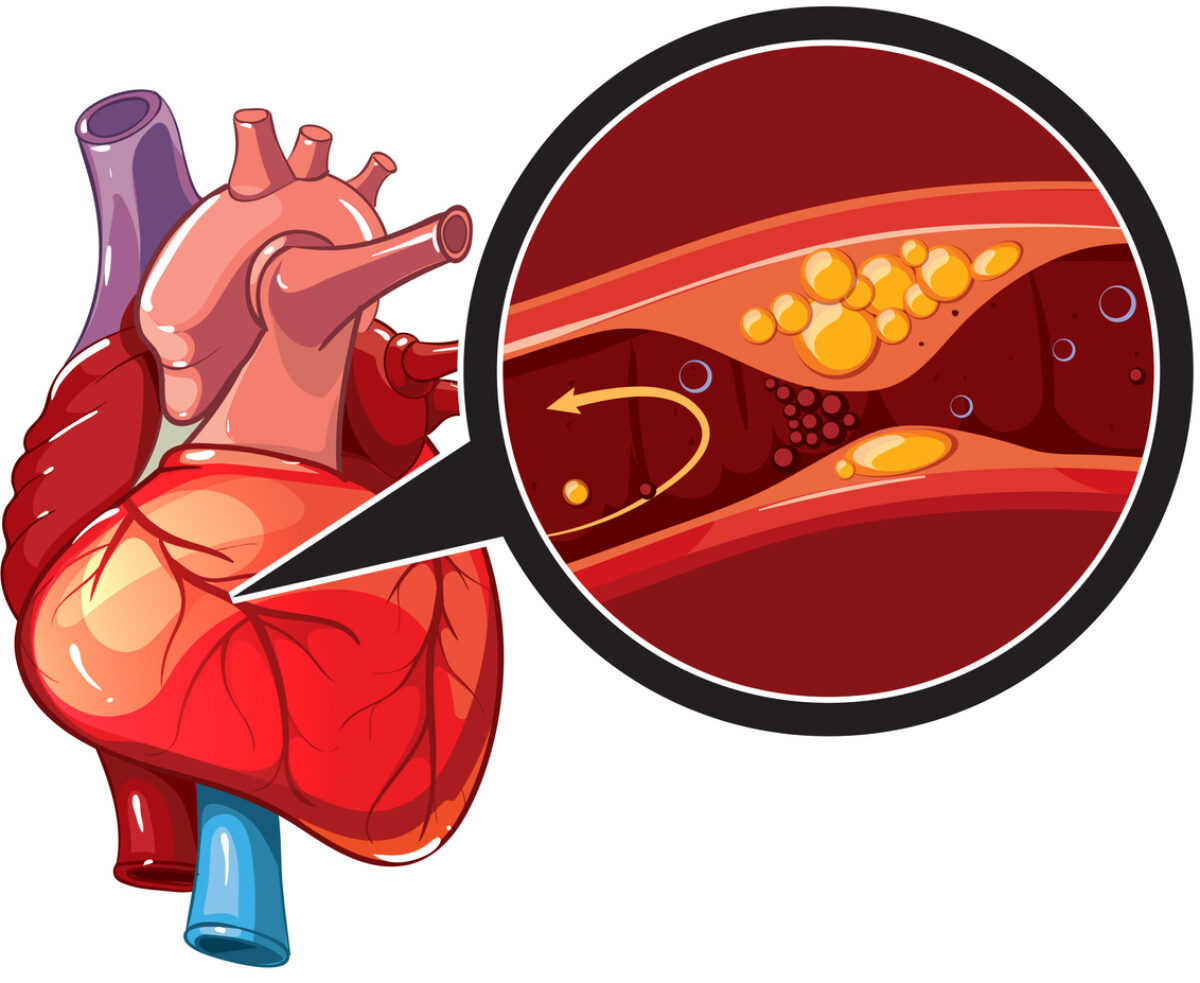
Heart blockage is one of the leading causes of heart attacks in India. heart blockage symptoms Most people do not realize they have a blockage until it becomes dangerous — sometimes 70%, 90%, or even fully blocked.
The good news? Your body gives early warning signs, but many people ignore them, assuming it’s acidity, stress, or tiredness.
This blog explains the 8 early symptoms of heart blockage, the causes, and when to see a cardiologist in Kolkata for immediate testing. heart blockage symptoms
❤️ 1. Chest Pain or Pressure That Feels Like “Weight” heart blockage symptoms
Chest pain due to blockage is NOT always sharp. Often, it feels like:
Tightness
Pressure
Burning
Heaviness
Pain may spread to the:
Left shoulder
Arm
Neck
Jaw
If this happens often, especially during walking, climbing stairs, or stress — it is a red flag.
❤️ 2. Shortness of Breath Even With Mild Activity heart blockage symptoms
If simple activities suddenly become hard, such as:
Walking
Taking stairs
Carrying bags
…it may indicate reduced blood flow due to blocked arteries.
❤️ 3. Fatigue or Unexplained Tiredness
A weak blood supply forces your heart to work harder, making you feel tired even after light activities. If fatigue becomes a daily companion, get your heart checked.
❤️ 4. Chest Burning Misunderstood as Acidity heart blockage symptoms
Many Indians confuse heart blockage pain with acidity. If your “gastric pain” occurs:
After walking
After stress
At night
With sweating
…it may not be acidity — it may be early heart blockage.
❤️ 5. Left Arm, Shoulder, or Jaw Pain heart blockage symptoms
Repeated pain or discomfort radiating to the left side of the body is a classic blockage symptom.
❤️ 6. Irregular Heartbeat or Palpitations
Blockage reduces oxygen supply to the heart muscles, causing:
Fast heartbeat
Skipped beats
Fluttering sensations
If you feel these frequently, consult a cardiologist immediately.
❤️ 7. Dizziness, Fainting, or Feeling Lightheaded
This happens when the heart can’t pump enough blood to the brain — another warning sign that arteries may be narrowing.
❤️ 8. Excessive Sweating Without Physical Activity
Sweating suddenly while resting or during chest discomfort is a common sign of unstable heart blood flow.
Heart attacks are rising rapidly in India — even among people in their 20s and 30s. The surprising truth? More than 80% of heart attacks are preventable with the right daily habits.
This blog gives you doctor-approved lifestyle changes that can strengthen your heart, lower your risk, and help you live longer — especially if you live in big cities like Kolkata where stress, pollution, and busy schedules affect heart health.
Let’s dive in.
❤️ 1. Start Your Day With a 20-Minute Walk prevent heart attack
Walking boosts your blood circulation, improves heart strength, and reduces cholesterol naturally.
Why it works:
Prevents artery blockage
Burns fat
Reduces stress hormones
Improves blood pressure
Even a simple morning walk in your neighborhood can lower your heart attack risk by 30–40%.
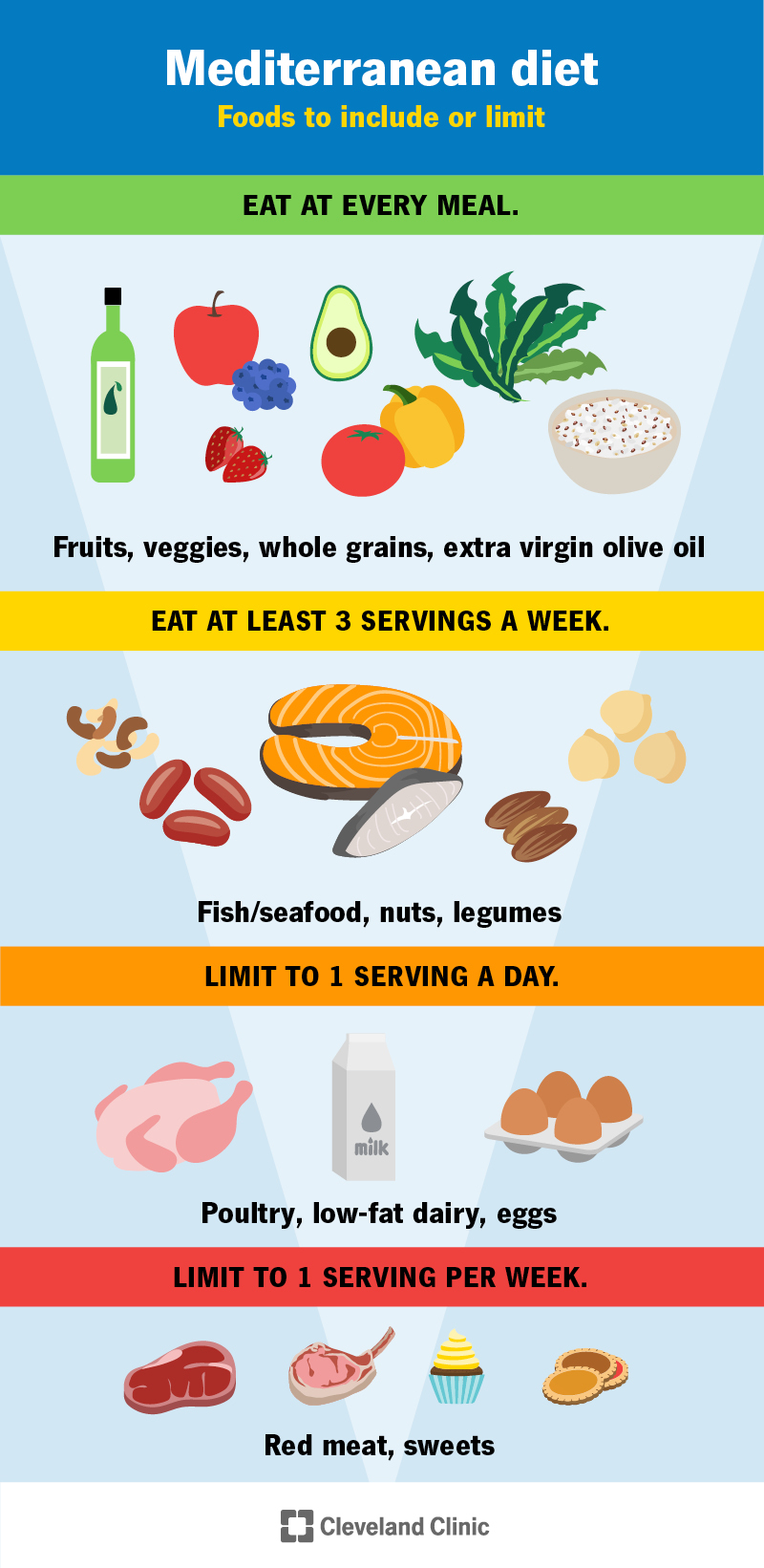
❤️ 2. Switch to a Heart-Safe Diet (Small Tweaks = Big Impact) prevent heart attack
A heart-friendly plate should include:
✔ Fruits & vegetables ✔ Whole grains ✔ Almonds, walnuts ✔ Lean protein (fish, chicken, sprouts) ✔ Olive or mustard oil ✔ Limited sugar and salt
Foods to reduce:
Fried snacks
Processed foods
Red meat
Sugary desserts
Trans fat items (bakery, packaged chips)
❤️ 3. Check Your BP & Sugar Every Month prevent heart attack
High BP and diabetes are the silent killers behind most heart attacks in India.
If you have:
BP above 130/80
Fasting sugar above 100
Family history of heart problems
You MUST be extra careful and consult a cardiologist near you for regular monitoring.
Heart disease doesn’t always come with dramatic chest pain. Many people in Kolkata ignore the early signs until it’s too late. Recognizing the symptoms early and meeting the right cardiologist in Kolkata can literally save your life. signs of heart disease
If you or someone you love has been “feeling something wrong” lately — read this before you ignore another symptom.
❤️ 1. Chest Pain or Pressure That Comes and Goes
Chest heaviness, burning, tightness, or pressure… even if mild… is a major warning sign. Never assume it’s acidity or stress.
If you feel chest discomfort more than once a week — see a heart specialist immediately.
❤️ 2. Shortness of Breath While Walking or Talking
If climbing stairs or walking short distances suddenly feels difficult, this may indicate:
Weak heart function
Blocked arteries
Valve problems
This is one of the most common early signs cardiologists see in Kolkata patients.
❤️ 3. Irregular Heartbeat or Sudden Palpitations
Feeling like your heart is “skipping beats” or “beating too fast” can indicate arrhythmia — a condition requiring urgent evaluation.
❤️ 4. Swelling in Legs, Ankles, or Feet
Fluid buildup may mean your heart isn’t pumping properly — a classic symptom of heart failure.
❤️ 5. Constant Fatigue or Feeling Tired Without Reason
If daily activities suddenly feel exhausting, your heart may not be supplying enough oxygen to your body.
❤️ 6. High BP or Diabetes That Is Hard to Control
In Kolkata, many patients ignore these conditions thinking medicine is enough. But uncontrolled BP/diabetes silently damages the heart and arteries.
A cardiologist should monitor you regularly.
❤️ 7. Family History of Heart Disease
If your parents or siblings had heart attacks, blockages, or sudden cardiac death before 55–60, your risk is 2–4x higher.
Testing early can prevent emergencies.
❤️ 8. Chest Pain During Stress or Exercise
Pain triggered during walking, climbing stairs, or emotional stress is a strong sign of coronary artery blockage.
Do NOT delay tests.
❤️ 9. Dizziness, Fainting, or Blackout Episodes
These symptoms may signal:
Valve disease
Rhythm disorders
Low blood flow to the brain
All require urgent heart evaluation.
❤️ 10. You Had COVID & Now Feel Heart Symptoms
Many people in Kolkata suffer post-COVID heart issues like:
Breathlessness
Tachycardia
Chest pain
Weakness
Post-COVID cardiac screening is extremely important. signs of heart disease
⭐ Why Choosing the Right Cardiologist Matters
Not all heart problems require surgery. Modern cardiology offers non-surgical, minimally invasive treatments like:
Heart disease continues to be one of the leading causes of death in India, and early diagnosis by an expert heart specialist can save lives. When you begin experiencing symptoms like chest pain, palpitations, shortness of breath, or unusual fatigue, searching for the best cardiologist in Kolkata becomes essential.
But with so many specialists available, how do you make the right choice?
This guide brings you everything you need to know — from understanding cardiology treatments to choosing the right expert, and why Dr. Avishek Saha is emerging as one of the most trusted interventional cardiologists in Kolkata.
❤️ What Does a Cardiologist Do?
A cardiologist is a specialist doctor who diagnoses and treats:
Heart attacks
Coronary artery disease
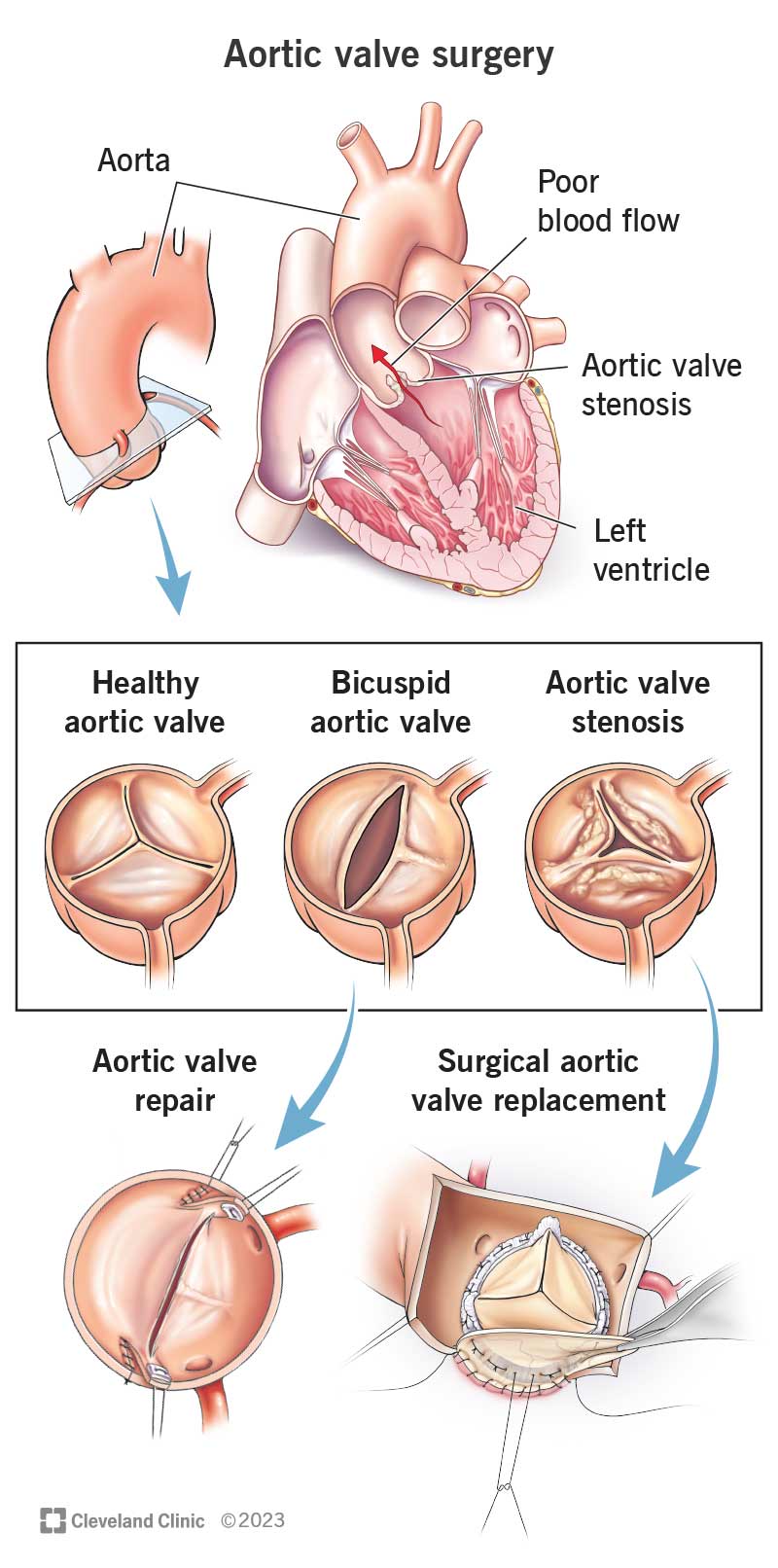
Valve diseases
Rhythm disorders
Congenital heart defects
Heart failure
High blood pressure
When a cardiologist is also trained in procedures like angioplasty, stent placement, device closure, or non-surgical valve interventions, they are known as an interventional cardiologist.
🔍 Top Signs You Should See a Cardiologist Immediately Cardiologist in Kolkata
Chest pain or tightness
Breathlessness while walking or climbing stairs
Irregular heartbeat or palpitations
Swelling in legs
Uncontrolled BP or diabetes
Family history of heart disease
Recovery after an angioplasty or surgery
If you experience these symptoms, search for a “cardiologist near me Kolkata” and book a consultation.
🏥 Why Choose an Interventional Cardiologist in Kolkata? Cardiologist in Kolkata
Interventional cardiologists perform minimally invasive, non-surgical procedures that help diagnose and treat heart problems with less pain and faster recovery.
Popular treatments include:
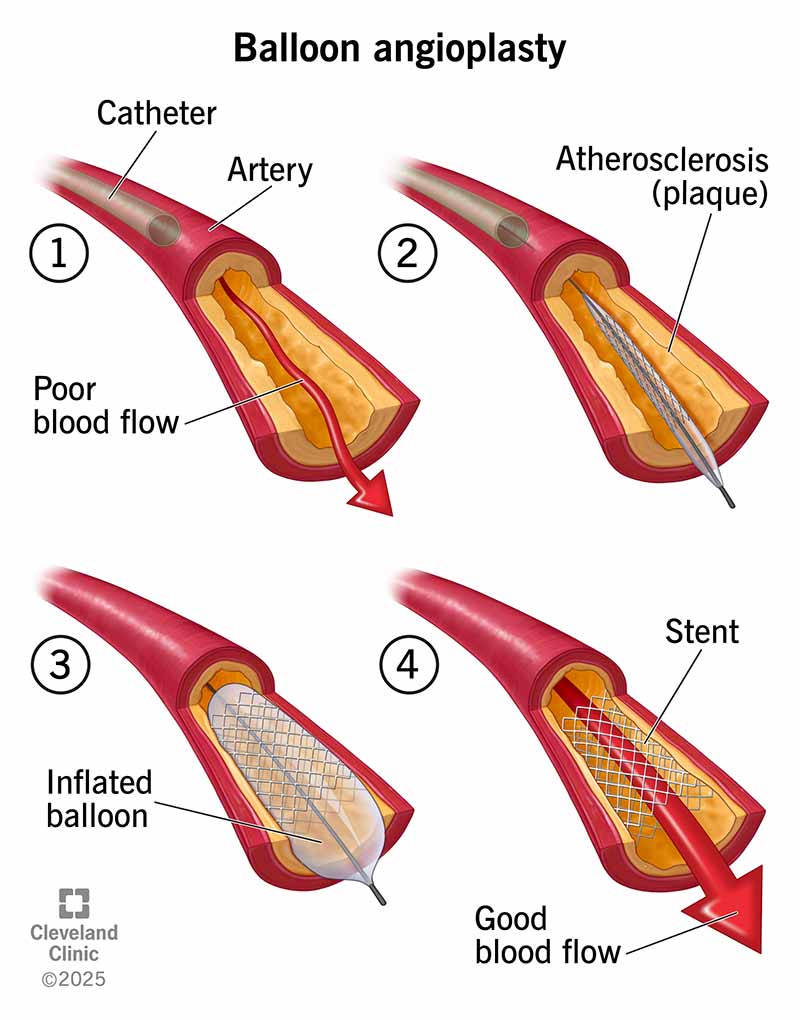
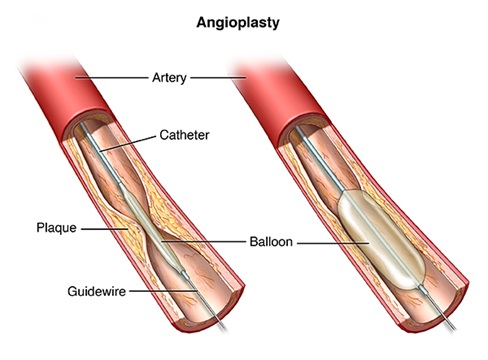
✔ Angioplasty & Stent Placement
Opens blocked arteries using a balloon and stent.
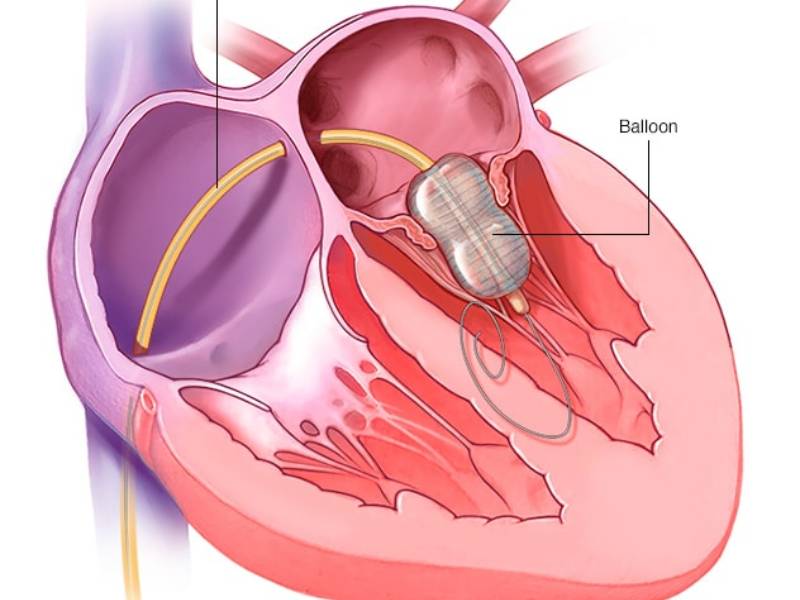
✔ Balloon Mitral Valvuloplasty (BMV)
A non-surgical alternative to open-heart surgery for mitral stenosis.
✔ Pacemaker / ICD Implantation
✔ Device Closure for ASD, VSD, PDA
Treats structural heart defects without open surgery.
✔ Peripheral Angioplasty
For blocked leg arteries.
Kolkata is now known as a major hub for advanced cardiology treatments with success rates comparable to global standards.
💗 BMV: A Breakthrough Alternative to Open-Heart Surgery
If you or a family member has Mitral Stenosis, you may not always need open-heart surgery. Balloon Mitral Valvotomy (BMV) is a safer, quicker and less painful option.
🔹 Benefits of BMV
No open chest incision
Faster recovery
Same-day or next-day discharge
Lower cost
Highly effective when done by experienced specialists
This is one of the signature expertise areas highlighted on the official cardiology page of 👉 dravisheksaha.com/cardiologist
📍 Finding the Best Cardiologist in Kolkata by Location Cardiologist in Kolkata
Searches like:
“cardiologist in Salt Lake Kolkata”
“cardiologist in South Kolkata”
“heart specialist in Mukundapur”
“interventional cardiologist near me Kolkata”
show that patients prefer specialists closest to their residence.
Kolkata has strong medical zones like Salt Lake, Mukundapur, Alipore, Garia, EM Bypass, and New Town — with leading hospitals and modern cath-labs.
⭐ Why Many Patients Prefer Dr. Avishek Saha Cardiologist in Kolkata
(Optimized for your website)
Dr. Avishek Saha is a leading Interventional & Structural Heart Cardiologist in Kolkata, known for:
Expertise in minimally invasive heart procedures
Trained in advanced structural heart interventions
Excellent patient communication
Emergency and critical cardiac care
Treatments across leading hospitals in the city
His website provides a well-structured guide on: ✔ Cardiologist selection ✔ Heart disease symptoms ✔ Non-surgical treatment options ✔ Location-based cardiology services in Kolkata
Visit: dravisheksaha.com/cardiologist
📈 Cost of Common Cardiology Procedures in Kolkata (Approx.) Cardiologist in Kolkata
(Good for SEO & user engagement)
Angioplasty: ₹65,000 – ₹2,00,000
Stent (DES): ₹28,000 – ₹40,000 per stent
Pacemaker: ₹55,000 – ₹2,50,000
BMV procedure: ₹55,000 – ₹80,000
Device closure (ASD/VSD): ₹1,00,000 – ₹3,00,000
Actual cost depends on hospital, device type, and patient condition.
📝 How to Choose the Best Cardiologist in Kolkata (Checklist) Cardiologist in Kolkata
✔ Check specialization (Interventional vs General) ✔ See hospital affiliations ✔ Compare treatment success rates ✔ Look for emergency availability ✔ Read patient reviews ✔ Consider proximity to your home ✔ Ensure the doctor handles your specific condition (valve disease, blockages, arrhythmia, etc.)
🧠 Top Google-Search FAQs Answered
1. Who is the best cardiologist in Kolkata?
It depends on your condition. For angioplasty, BMV, device closure, and structural heart disease, choose an interventional cardiologist trained in complex procedures.
2. Is angioplasty safe?
Yes, when performed by an experienced specialist in a modern cath-lab.
3. What is the best alternative to open-heart surgery?
Balloon Mitral Valvotomy (BMV), TAVR/TMVR, and device closures are non-surgical alternatives depending on the condition.
4. How soon should I see a cardiologist?
Immediately if you experience chest pain, breathlessness, or palpitations.
📌 Conclusion: Your Heart Deserves Expert Care Cardiologist in Kolkata
Finding the right cardiologist in Kolkata can prevent major emergencies, improve quality of life, and ensure long-term heart health. Interventional experts like Dr. Avishek Saha are transforming cardiac care through modern, minimally invasive treatments.
When it comes to your heart, “good” isn’t enough. You want the best. Every day, thousands of patients search for the “Top 10 heart specialist doctor in Kolkata” or the “Best cardiologist doctor list in Kolkata.” The search results often throw up a confusing mix of big hospital names like Apollo, BM Birla, and Manipal. heart specialist doctor in Kolkata
But here is the truth: The “No. 1” cardiologist isn’t just a rank on a list. It is the doctor who is available when you need them, transparent about costs, and skilled in saving lives.
If you are confused by the endless lists, this guide will help you cut through the noise and find the right heart specialist for you or your parents.
The “Big Hospital” Trap: Apollo vs. Manipal vs. Specialized Clinics heart specialist doctor in Kolkata
Many patients instinctively search for a “Cardiologist in Apollo Kolkata” or “BM Birla” because of the brand name. These hospitals undoubtedly have excellent infrastructure. However, big hospitals often come with:
Long waiting times for appointments.
Rotating doctors (you might not see the same senior consultant every time).
Higher procedure costs.
The Better Alternative: Leading Interventional Cardiologists like Dr. Avishek Saha often practice at top-tier hospitals (like Manipal Hospital, Mukundapur and Woodlands) but also run specialized private clinics.
Benefit: You get the safety of a big hospital’s OT for surgeries (Angioplasty/Pacemaker) but the personalized care and accessibility of a private clinic for consultations.
Who is the No. 1 Cardiologist in Kolkata?
There is no single “No. 1” because cardiology has many sub-specialties. When creating your own best cardiologist doctor list in Kolkata, look for a specialist based on your specific need:
For Angiography & Angioplasty (Interventional): You need a doctor with high volume experience. Dr. Avishek Saha has performed over 1,500 successful angioplasties and specializes in complex radial (wrist) procedures.
For Irregular Heartbeats (Devices): Look for experts in Pacemaker and ICD implantation.
For Structural Defects: Specialists who handle ASD/VSD device closures.
Dr. Saha’s Advantage: He covers all three verticals, making him a “One-Stop” expert for complex cardiac care.
“Cardiologist Kolkata Near Me”: Why Location Matters heart specialist doctor in Kolkata
In a heart attack, time is muscle. If you live in South Kolkata (Alipore, Kalighat, Tollygunge) or East Kolkata (Mukundapur, Salt Lake), traveling 2 hours to a doctor in North Kolkata is risky.
Dr. Avishek Saha has strategically located his clinics to be the “Best Cardiologist Kolkata Near Me” for a vast majority of the city:
Manipal Hospital (Mukundapur): For East Kolkata & Bypass residents.
Woodlands & Alipore: For South Kolkata residents.
IRIS Hospital (Ganguly Bagan): For Garia/Jadavpur residents.
5 Signs You Have Found the “Best” Doctor
Forget the internet rankings for a moment. The best doctor is one who:
Listens: Does not rush you out in 5 minutes.
Explains: Uses simple language, not medical jargon (e.g., explaining why you need a stent vs. bypass).
Transparent:Discusses the cost of stents (Drug-Eluting Stents) and packages openly.
Accessible: Is available for emergencies, not just appointment slots.
Technologically Advanced: Uses modern techniques like Radial Angiography (via wrist) which is less painful and allows quicker discharge.
Conclusion: Trust Experience Over Lists heart specialist doctor in Kolkata
While it is helpful to look at the top 5cardiologist in Kolkata lists, your decision should be based on trust and expertise.
Whether you need a routine check-up, a second opinion on Angioplasty, or urgent care, Dr. Avishek Saha offers the perfect blend of world-class interventional skills and the compassionate “human touch” that patients often miss in large corporate setups.
I. Executive Summary: The Agitation-Relief Conversion Funnel for Mitral Stenosis BMV procedure specialist Kolkata
The following content strategy is meticulously designed to capture high-intent patients diagnosed with Mitral Stenosis (MS) who are currently immobilized by fear of traditional treatment protocols. The standard expectation for severe heart valve intervention is Open-Heart Surgery (OHS), a procedure associated with significant patient anxiety due to its invasive nature and mandated recovery period. The strategic objective is to leverage this anxiety—the Agitation phase—by validating the patient’s worst fears regarding OHS complexity and then providing an immediate, data-backed resolution—the Relief phase—through the introduction of Balloon Mitral Valvuloplasty (BMV). BMV procedure specialist Kolkata
The friction point exploited within this content architecture is the acute trauma associated with the OHS recovery timeline, specifically the 6-8 week recovery period involving limited physical activity, and the invasiveness of the Median Sternotomy (cutting through the breastbone). By confirming the validity of these concerns, the content establishes immediate trust and empathy with the reader.
The rapid strategic pivot to BMV offers quantifiable relief. Data confirms that BMV allows for rapid discharge, often within 24-48 hours, and presents a significantly lower procedural mortality rate. This dramatic contrast establishes BMV not merely as an alternative, but as a clinically advantageous option for eligible candidates. The narrative is engineered to rank aggressively for comparison queries (“Alternatives to open-heart surgery for MS”), positioning Dr. Saha, a specialist in structural heart intervention, as the definitive solution provider for high-quality, minimally disruptive valve care.
The content structure directly mirrors the patient’s internal crisis: recognizing the urgency of the condition (MS progression), confronting the terrifying perceived treatment (OHS), and initiating a search for a better way (alternatives). This emotional congruence ensures that once the post is discovered, the compelling evidence of minimal disruption offered by BMV translates into high lead conversion rates. The ultimate goal is to generate consultations for an eligibility assessment, capitalizing on the patient’s newfound confidence in a specialized, less invasive pathway.
II. Strategic Context and Target Audience Mapping BMV procedure specialist Kolkata
A. Defining the Mitral Stenosis Patient Journey: From Diagnosis Anxiety to Treatment Decision
Mitral Stenosis is a serious, progressive condition requiring timely intervention. While heart valve issues are often generalized as ailments of advanced age, the primary cause of MS globally is Rheumatic Heart Disease (RHD), a condition that frequently affects younger adults. This demographic is critically sensitive to the duration and severity of recovery time, as prolonged physical limitations impact their careers, financial stability, and active lifestyles.
The clinical necessity for intervention accelerates the patient’s search behavior. MS symptoms, such as fatigue and shortness of breath, worsen over time. Critically, untreated MS quickly escalates the risk of severe secondary conditions, including pulmonary hypertension, Atrial Fibrillation (AFib), and Congestive Heart Failure (CHF). The decision to seek treatment is often made under duress, driven by worsening symptoms that signal imminent danger. This urgency means patients are seeking a resolution immediately, but the traditional intervention (OHS) presents a seemingly insurmountable obstacle—a massive life interruption—creating the strategic friction necessary for the content to drive conversion.
B. Targeting MoFu Keywords: Capturing Patients Comparing OHS vs. Non-Surgical Options
The content strategy is intentionally focused on the Middle-of-Funnel (MoFu) and Bottom-of-Funnel (BoFu) stages, targeting searchers who have already received a diagnosis and are actively evaluating treatment methods. These high-intent users employ comparison queries, signaling a readiness to select a provider once a viable alternative to OHS is found.
The content outline is structured explicitly to align with these high-value search terms. Phrases such as “Mitral stenosis surgery vs BMV” and “Alternatives to open-heart surgery for MS” must be prominently featured in headings, subheadings, and introductory paragraphs. Capturing these comparison queries ensures that the post intercepts the patient at the precise moment of decision-making, offering the most compelling data set to resolve their procedural anxiety.
C. The Emotional Pain Point: Deconstructing Patient Fear of Median Sternotomy and Prolonged Recovery BMV procedure specialist Kolkata
The primary psychological obstacle preventing MS patients from moving forward with OHS is not necessarily the risk of the procedure itself, but the associated physical trauma and required recovery. The content must acknowledge and validate the fear surrounding the median sternotomy, which requires physically cutting through the breastbone to access the heart. This invasive component serves as the central psychological anchor for patient anxiety, symbolizing pain, extensive scarring, and physical vulnerability.
Furthermore, the post must emphasize the magnitude of the post-OHS disruption: a mandated 6-8 weeks of limited physical activity. For the RHD patient demographic, which may include younger, career-focused individuals, this mandated rest period translates directly into severe economic stress, loss of professional momentum, and a dependence on caregivers. The content’s strategy is founded on the recognition that the patient’s core fear is the loss of self-sufficiency and economic stability for those two months. By articulating this disruption, the content establishes profound empathy. In turn, BMV’s rapid return to activities is positioned not just as a clinical advantage, but as a critical economic and quality-of-life benefit that outweighs the traditional surgical path. The specialized content is, therefore, selling restored time and freedom alongside superior clinical outcomes.
III. Agitation Section: Facing the Reality of Open-Heart Surgery (OHS) BMV procedure specialist Kolkata
The Agitation Section must clearly, yet respectfully, lay out the facts regarding OHS to create the emotional imperative for seeking an alternative. This section serves to justify the patient’s existing fear, preparing them for the pivot to relief.
A. Anatomy of Invasive Surgery: General Anesthesia and the Need for Bypass Support BMV procedure specialist Kolkata
OHS is a major surgical event demanding a high level of patient preparation and tolerance. It necessitates deep General Anesthesia. For many patients, the associated risks and post-operative side effects of general anesthesia constitute a significant source of anxiety that compounds the fear of the physical procedure itself. The complexity of the operation is fundamentally tied to the necessity of physical access.
The defining characteristic of OHS is the requirement for a sternotomy. This process involves the physical splitting of the sternum (breastbone) to provide surgeons with direct visualization and access to the mitral valve. This severe trauma to the skeletal structure and surrounding tissue is the core differentiator from any percutaneous, minimally invasive procedure, leading directly to the prolonged recovery period.
B. The Cost of Recovery: Quantifying the 6-8 Week Disruption to Life and Work BMV procedure specialist Kolkata
The invasiveness of OHS dictates a long and mandatory recovery schedule. The initial hospital stay is typically lengthy, requiring 5-7 days of in-patient care. This duration acts as a qualitative marker of the sheer severity and trauma inflicted by the procedure.
The most critical data point for the patient is the required recovery outside the hospital: a mandated 6-8 week period of severely limited physical activity. The narrative must focus on the tangible, disruptive implications of this mandate: the patient will be temporarily unable to drive, prohibited from lifting weights exceeding a few pounds (making simple tasks like lifting children or groceries impossible), and often unable to perform demanding work tasks. This required two-month operational delay validates the patient’s fear of lost independence and financial strain, amplifying the urgent need for a faster solution.
C. Mitral Stenosis: Why Waiting for Symptoms to Worsen is Not a Strategy BMV procedure specialist Kolkata
The strategic framing must acknowledge that the pain of OHS recovery is magnified by the knowledge that delaying treatment is dangerous. Patients are often trapped between the urgency of their deteriorating condition and the fear of massive surgery.
Clinical messaging must emphasize that MS is progressive. Delaying treatment due to OHS fear is medically unsound, as it rapidly advances the risk of critical secondary heart conditions like CHF and AFib. Symptoms like fatigue and shortness of breath are clear indicators of this relentless progression. By establishing OHS as the source of a two-month delay, the content underscores the appeal of BMV’s speed and minimal disruption, as it allows the patient to address the dangerous progression of their condition without incurring a significant temporary sacrifice of their quality of life.
IV. The Definitive Pivot: Introducing Balloon Mitral Valvuloplasty (BMV)
The transition to BMV must be executed as the logical, data-driven counterpoint to OHS, focusing on precision, speed, and reduced trauma.
A. A Revolutionary Approach: Percutaneous Access and Minimally Invasive Excellence
Balloon Mitral Valvuloplasty represents a paradigm shift in structural heart care. Unlike OHS, BMV is a percutaneous procedure. This means access to the heart valve is gained through a small puncture, typically in the groin, using a catheter. This approach entirely avoids the necessity of a median sternotomy and the associated trauma to the chest cavity.
This minimally invasive technique also substantially reduces the risk associated with anesthesia. While OHS mandates deep general anesthesia, BMV procedures often utilize only local anesthesia or conscious sedation. This directly addresses a major source of patient anxiety—the fear of being “put under”—further distinguishing BMV as a superior, low-impact option for eligible patients.
B. The Mechanics of Restoration: How the Specialized Balloon Corrects Fused Commissures
To build patient confidence, the content must clearly define the technical efficacy of BMV. The procedure is highly targeted; a specialized balloon catheter is navigated to the mitral valve. The mechanism involves the controlled inflation of this balloon to physically and definitively split the fused mitral valve commissures. This surgical precision, achieved through minimal access, reassures the patient that the low invasiveness does not compromise the anatomical correction required to restore valve function.
The clinical success of this targeted approach is profound. Successful BMV delivers immediate and sustained hemodynamic and symptomatic improvement. The ability of the procedure to yield almost instantaneous functional benefits validates the high-tech, targeted nature of the solution, establishing a stark contrast with the blunt force implied by traditional surgery.
C. Identifying BMV Eligibility: When is Minimally Invasive Intervention Possible?
It is crucial to set accurate expectations regarding candidacy. BMV is highly effective, but its suitability is dependent on specific anatomical factors, such as the flexibility of the valve leaflets and the degree of calcium accumulation. Not all MS patients are candidates for this less invasive method.
This subsection serves as the primary conversion trigger. By emphasizing that determining anatomical suitability requires advanced diagnostic imaging and assessment by an expert Structural Heart Interventionist (such as Dr. Saha), the content clearly defines the necessary next step. The specialized solution is available, but the expert consultation is mandatory for personalized risk stratification and anatomical mapping.
V. Data-Driven Comparison: OHS vs. BMV (The Conversion Engine)
This section provides the objective, quantifiable evidence required to shift the patient’s decision firmly toward the minimally invasive route. Presenting this information in a clear, comparative matrix format maximizes impact and readability.
A. Procedure Comparison Matrix
The following table serves as the central piece of evidence, neutralizing anxiety with concrete data points comparing the two procedures:
Mitral Stenosis Intervention: OHS vs. BMV Comparison
A common patient assumption is that a less invasive procedure carries a higher inherent risk. The data decisively refutes this. The content must directly cite the lower risk profile associated with BMV. Procedural mortality for BMV is highly favorable, typically ranging from 0-1%. This compares significantly well against the mortality rate associated with Mitral Valve Replacement (MVR) via OHS, which is often cited as 2-5%.
This objective safety data neutralizes the patient’s primary fear that choosing the easier recovery path means accepting greater clinical risk. For eligible candidates, the evidence suggests the opposite: BMV offers a safer pathway with minimized physical trauma. This quantitative advantage is essential for securing patient confidence.
C. Analyzing Patient Quality of Life (QoL) Data Post-Intervention
The most persuasive argument for BMV rests on the restoration of quality of life and speed of return to normal function. The mandatory 5-7 day hospital stay following OHS is contrasted sharply with the routine 24-48 hour discharge achievable after BMV. This reduction in hospitalization is a powerful signal of reduced procedural impact.
The most powerful metric is the activity restoration timeline. The ability for patients to return to normal activities often within days post-BMV must be repeatedly juxtaposed against the 6-8 weeks of required physical inactivity imposed by OHS. The patient is calculating the risk-reward ratio, and the data suggests that with BMV, the risk is lower (0-1% mortality) and the reward (restored activity and time) is dramatically faster. This combination creates a scenario that overwhelmingly favors the minimally invasive pathway for appropriate candidates.
VI. Establishing Dr. Saha’s Structural Heart Authority BMV procedure specialist Kolkata
The decision to pursue a less common, specialized intervention like BMV is inherently tied to the perceived competence and specialization of the physician. The content must clearly establish Dr. Saha’s authority to build the necessary trust.
A. Why Expertise Matters: The Complexity of Structural Heart Intervention (SHI)
BMV is not a routine procedure within general cardiology. It is classified as a high-level Structural Heart Intervention (SHI). This distinction is critical because it signifies that the successful execution of BMV demands specific, advanced training far exceeding that of general cardiologists or even general cardiovascular surgeons.
Successful BMV requires immense precision. The procedure necessitates advanced expertise in complex percutaneous vascular access (PVI) and meticulous navigation of the catheter to achieve the optimal splitting of the fused commissures. By detailing these technical requirements, the content transforms the specialist’s expertise from a simple qualification into a guarantee of quality and precision. This reassurance is vital for patients seeking a high-quality outcome from a less invasive method.
B. Case Studies and Technical Proficiency: Highlighting Experience
The narrative must convey that Dr. Saha’s technical mastery is the direct mechanism by which patients achieve the minimal disruption and rapid recovery touted by the comparison data. Proficiency in handling structurally complex cases, particularly those arising from Rheumatic Heart Disease, is essential to building confidence.
Positioning the practice as a leader in delivering immediate and sustained symptomatic improvement through BMV reinforces the value proposition. The specialist’s experience in SHI ensures that the high-tech, targeted correction of the valve commissures is executed with the highest degree of safety and efficacy, transforming the patient’s hope into reasoned confidence.
C. Addressing Patient Concerns: Eligibility Assessment and Risk Stratification
Skepticism surrounding minimally invasive options often centers on whether the patient is truly a suitable candidate. The content must emphasize the professional responsibility of the specialist. Dr. Saha’s team utilizes detailed, advanced diagnostics—including anatomical mapping and imaging—to accurately and ethically assess BMV candidacy.
This approach ensures that the procedure is only recommended when anatomically appropriate and clinically advantageous, solidifying the specialist’s role as a trusted advisor, not merely a technician. The ultimate decision point is the consultation, where the patient’s unique anatomy and clinical situation are evaluated against the specialist’s extensive experience, leading directly to the most appropriate, least disruptive treatment path.
VII. SEO Implementation Strategy and Optimization Tactics
The strategic effectiveness of this content hinges on its ability to dominate the SERP for highly transactional comparison queries, ensuring the patient finds the definitive answer at the moment of peak intent.
A. Target Keyword Cluster Map
The primary focus remains on High-Intent MoFu/BoFu Keywords. The content must prioritize explicit comparison phrases identified in the research, such as “Alternatives to open-heart surgery for MS,” “Mitral stenosis surgery vs BMV,” and “Non-surgical mitral stenosis treatment”. The strategic advantage is gained by intercepting the patient at the moment of decision-making.
Furthermore, Latent Semantic Indexing (LSI) must be achieved through the dense, organic coverage of related clinical terms, including “rheumatic heart disease,” “percutaneous valvuloplasty,” “sternotomy recovery,” and “hemodynamic improvement”. This comprehensive terminology builds authority and improves search engine understanding of the page’s topical depth.
B. On-Page Optimization Checklist
The structuring of the content must be optimized for search engine clarity and user experience. The content should utilize clear H2 and H3 tags that explicitly incorporate the core comparison phrases and critical recovery metrics. Examples include strategic headers like “6-8 Weeks vs. Days: The Recovery Time Difference” and “The Reduced Risk Profile: Comparing 0-1% Mortality to 2-5%.”
Crucially, Section V, which contains the Comparative Matrix, must be meticulously optimized for Google’s featured snippets. This involves ensuring that the recovery timelines (24-48 hours versus 6-8 weeks) and the mortality data points (0-1% versus 2-5%) are presented in easily extractable formats. By providing a definitive, authoritative, and clinically sourced comparison, the page increases its likelihood of ranking prominently for transactional queries, making it the final, reliable source for the patient’s decision. BMV procedure specialist Kolkata
VIII. Conversion Architecture and Next Steps
A. Deployment of High-Value CTAs: Scheduling an Eligibility Consultation BMV procedure specialist Kolkata
The objective of this high-intent content is consultation booking. The Primary Call-to-Action (CTA) language must on the low-commitment, high-value step of assessing candidacy, specifically: “Determine Your Eligibility: Schedule a Consultation with Dr. Saha, Structural Heart Expert.”
CTAs must be strategically placed immediately following the critical decision points, specifically after the eligibility criteria section (IV.C) and at the final conclusion. These placements ensure that once the patient is convinced of the clinical and lifestyle advantages, the conversion mechanism is immediately accessible. BMV procedure specialist Kolkata
B. Lead Nurturing Strategy for BMV Prospects
To capture and nurture potential patients who require more time for research, a secondary, softer CTA should be integrated. A resource download offer, such as “Download Your Checklist: The First 7 Days Post-BMV,” serves two strategic purposes: reinforcing the dramatically rapid recovery timeline and capturing essential email leads for future communication. This lead magnet subtly reinforces the reality that post-BMV recovery is measured in days, not months. BMV procedure specialist Kolkata
C. Conclusion: Trading Fear for Freedom BMV procedure specialist Kolkata
The conclusion must synthesize the entire strategic rationale into an emotionally empowering mandate. Patients suffering from Mitral Stenosis no longer have to reconcile the urgency of their condition with the trauma and prolonged 6-8 week disruption of traditional OHS. Instead, they can achieve immediate symptomatic improvement and rapid recovery, often returning to normal life within days, under the specialized care of a structural heart intervention expert. The concluding message should be decisive: the choice is no longer between sickness and sacrifice, but between an outdated, highly invasive procedure and a specialized, evidence-backed pathway to rapid health restoration. BMV procedure specialist Kolkata
I. The Crisis in Your Calves: Chronic Leg Pain as a Ticking Cardiovascular Bomb atypical heart attack symptoms kolkata
A. The Deceptive Silence of Peripheral Artery Disease (PAD)
Chronic leg pain—often characterized by aching, fatigue, or cramping known medically as claudication—is an alarm bell that is frequently silenced by patient inertia and, critically, by general medical practitioners. It is common for individuals, particularly those in older age groups, to dismiss these symptoms as merely a routine component of the aging process or minor orthopedic issues. This persistent dismissal, however, allows a silent and deadly cardiovascular condition to advance undetected: Peripheral Artery Disease (PAD). atypical heart attack symptoms kolkata
PAD is far more than just discomfort in the legs; it is a profound failure of the body’s circulation system, specifically the narrowing or blockage of arteries supplying blood to the lower extremities, usually caused by atherosclerosis—the buildup of fatty plaque inside vessel walls. The failure to recognize these early warning signs has contributed to an escalating global health crisis. Data from the Global Burden of Disease study reveals that global cases of PAD surged dramatically, climbing from approximately 66 million in 1990 to more than 113 million in 2019. This massive and growing prevalence underscores the urgency required in diagnosis and intervention.
The most critical factor overlooked when chronic leg pain is generalized is that PAD is universally classified by medical guidelines as a major cardiovascular disease, not merely a localized limb problem. The pathological process of atherosclerosis that restricts blood flow in the legs often affects the coronary and carotid arteries simultaneously. Large-scale studies conclusively demonstrate that individuals diagnosed with PAD have a significantly higher concomitant risk of experiencing a heart attack or stroke. This understanding reveals a vital clinical principle: chronic leg pain is the visible sign of a hidden, deadly, systemic disease. A patient who perceives only localized discomfort is failing to address a systemic cardiovascular time bomb. Therefore, the failure to screen aggressively for PAD in high-risk patients equates to a failure to screen for imminent cardiac disaster, dramatically escalating the threat level and mandating urgent consultation with a specialist. atypical heart attack symptoms kolkata
B. Understanding the Spectrum of PAD Progression atypical heart attack symptoms kolkata
The disease pathway of PAD is characterized by distinct stages, ranging from mild states, which may be asymptomatic or only cause claudication, to the most severe and limb-threatening forms. The most critical manifestation is Critical Limb Ischemia (CLI). CLI represents the terminal stage of PAD where blood flow is so severely restricted that the tissues cannot receive adequate oxygen and nutrients. In this state, devastating complications such as non-healing ulcers, severe infections, or gangrene can develop, placing the limb in immediate and high peril of amputation.
The progression from mild claudication to severe CLI highlights why early, specialist intervention is paramount. Timely diagnosis and the initiation of targeted treatment are absolutely crucial for halting the progression of the disease and preventing these long-term, irreversible complications. The goal of specialist care is to restore robust circulation well before the patient reaches the point of ischemic crisis, securing both limb health and overall cardiovascular prognosis.
II. The Misdiagnosis Trap: The Failure of General Care and the Amputation Catastrophe atypical heart attack symptoms kolkata
A. The Cost of Missed or Delayed Diagnosis
One of the most insidious dangers of PAD lies in its high rate of misdiagnosis or delayed recognition. Because the symptoms overlap with more common, less threatening conditions, many patients are often only correctly diagnosed after the disease has already progressed significantly. General practitioners frequently miss the connection between established underlying conditions—such as existing heart disease or chronic high blood pressure—and the subsequent development of PAD. This failure in detection places the patient on a path toward devastating outcomes.
The quantitative consequence of delayed or inconsistent care is staggering. Research tracking PAD patients highlights a critical link between the continuity of care and the risk of limb loss. Patients who experienced inconsistent access to necessary, high-quality vascular care, or who suffered delays in follow-up and intervention, were found to be significantly more likely to undergo catastrophic procedures. Specifically, these patients were nearly three times more likely to require a major amputation (Odds Ratio 2.96, 95% CI 2.51–3.50) and substantially more likely to require a minor amputation (Odds Ratio 2.48, 95% CI 2.29–2.65) compared to those receiving continuous care. This stark numerical increase in risk underscores the critical reality: the longer optimal, specialized intervention is delayed, the higher the mathematical certainty of limb loss becomes.
B. The Scale of the Amputation Epidemic atypical heart attack symptoms kolkata atypical heart attack symptoms kolkata
The clinical reality surrounding PAD is that amputation is not an unavoidable fate of the disease but, in many cases, a direct consequence of suboptimal care and systemic failure to implement evidence-based diagnostics and treatment protocols. PAD has earned the grim title of the “silent amputator” because it is the single largest cause of non-traumatic amputations. In the United States alone, PAD affects over 10 million individuals and contributes to approximately 400 amputations every single day. This translates to an alarming total of around 150,000 non-traumatic leg amputations annually.
What makes this epidemic particularly unacceptable is that a substantial proportion of these amputations are potentially preventable. Despite the existence of clear, evidence-based diagnostic and therapeutic approaches that can significantly reduce amputation risk, the implementation and patient adherence to these strategies remain suboptimal. This failure is most acutely observed in the highest-risk group: patients with diabetes, who account for the majority of non-traumatic amputations. Following a period of decline, amputation rates among diabetic patients shockingly increased by 50% between 2009 and 2015. This resurgence proves that general practice is often failing to deliver the optimal, life- and limb-saving management that is required. Therefore, the excessively high rate of amputation reflects a failure of implementation and care continuity, establishing that specialized, proactive intervention is urgently needed to interrupt this dangerous trend.
III. Your Personalized Warning: Mapping the High-Risk Profile atypical heart attack symptoms kolkata
Identifying and acting on high-risk factors is the essential first step in limb preservation. For individuals with chronic leg pain, recognizing specific co-morbidities transforms the general health warning into a highly relevant, urgent personal appeal.
A. The Acute Risk for the Diabetic Population
The link between Type 2 Diabetes Mellitus (T2DM) and PAD is profound, particularly within the target demographic. A recent systematic review and meta-analysis focusing on the Indian population confirmed that the combined prevalence of PAD among individuals with T2DM is a significant 18%. This means that nearly one in five diabetic patients in the region is affected by this circulatory crisis, justifying the immediate need for specialist consultation and diagnostic testing.
When assessed across various high-risk patient cohorts—including those with Ischemic Stroke (IS), Cardiovascular Disease (CVD), or Diabetes Mellitus (DM)—the overall prevalence of PAD detected by the Ankle-Brachial Index (ABI) was found to be 27.1%, with the prevalence being highest specifically among those with DM. Age and the duration of DM were consistent risk factors across all cohorts. Furthermore, demographic analysis indicates that the risk profile for this patient population is highly specific: for South Asians, diabetes, smoking, male sex, and mean systolic blood pressure were all independently associated with PAD. By understanding the elevated 18% prevalence among T2DM patients in the region , the post moves beyond being a general advisory and becomes a direct, hyper-relevant call to action, establishing the high likelihood of disease and justifying immediate specialized assessment.
B. The Pervasive Threat of Hypertension
Beyond diabetes, high blood pressure (hypertension) is recognized as a major independent force driving the arterial damage that precedes and exacerbates PAD. The causal mechanism is clear: high BP damages the delicate lining of the artery walls, accelerates the atherosclerotic process, and increases arterial stiffness. A landmark study in the Atherosclerosis Risk in Communities (ARIC) cohort found that people with hypertension had a 1.5 to 2 times higher risk of developing PAD compared to those with normal blood pressure levels. This data confirms that for patients managing hypertension, leg pain should never be dismissed; it is a signal that the ongoing arterial damage has reached the periphery.
C. The Imperative of Specialized Screening
Given the high prevalence and severe consequences, current medical consensus globally mandates specialized screening for PAD in high-risk groups. Specifically, screening using the Ankle-Brachial Index (ABI)—a non-invasive assessment comparing blood pressure in the ankle to the arm—should be routinely performed among patients with ischaemic stroke, cardiovascular disease, or diabetes mellitus.
For a patient reading this and recognizing their own risk factors (T2DM, hypertension, smoking history, or chronic leg pain), the critical question becomes: has my general practitioner performed this essential, life-saving screening? If the answer is no, the patient is almost certainly receiving suboptimal care. The specialist’s role begins precisely here—by moving beyond generalized assumptions of “old age” and providing the targeted, evidence-based vascular screening required to catch the disease before it leads to critical limb ischemia or amputation.
IV. The Pivot to Limb Preservation: Why Endovascular Treatment is Statistically Superior atypical heart attack symptoms kolkata
For patients facing chronic PAD, the choice of intervention is crucial, often representing the decisive factor between limb preservation and amputation. Advanced peripheral intervention specialists focus on techniques that are not merely minimally invasive, but maximally successful for long-term survival and limb salvage.
A. The Endovascular Advantage: Risk Reduction and Recovery
Dr. Avishek Saha specializes in advanced endovascular procedures—techniques performed through small vessel punctures to restore arterial blood flow (revascularization) with minimal patient trauma. This approach is scientifically substantiated to provide superior outcomes compared to traditional, highly invasive open surgical bypass.
Clinical studies demonstrate that an endovascular procedure is associated with a risk-adjusted 16% decreased risk of amputation or death when compared to open revascularization over the study period. This single data point—a 16% improvement in the combined metric of life and limb preservation—is the ultimate validation of the specialized approach. It confirms that endovascular care is not just about avoiding large incisions; it directly translates to improved life and limb survival rates. Beyond the mortality benefit, endovascular surgery provides significant advantages in terms of complication profile and recovery dynamics. It results in fewer complications, shorter hospital stays, and a lower overall mortality rate when compared with traditional open surgery, even while achieving similar rates of technical success and limb salvage.
B. Amplified Benefit for Complex Cases
The benefits of the endovascular approach are particularly pronounced where the patient risk is highest. The amputation-free survival benefit associated with endovascular revascularization was found to be significantly more pronounced in patients with complex co-morbidities, such as congestive heart failure (CHF) or ischemic heart disease (IHD), than in those without these conditions. This suggests that the specialized, less traumatic nature of endovascular techniques provides essential protection for patients whose systemic health status might make them poor candidates for major open surgery.
Furthermore, for the most severely affected patients—those who have already progressed to Critical Limb Ischemia (CLI)—the amputation-free survival benefit associated with an endovascular approach persisted, proving its efficacy precisely at the point of greatest danger. While endovascular procedures may sometimes require more vigilant, ongoing maintenance (with a slightly higher rate of subsequent intervention compared to open surgery—7.4% greater at 30 days) , this reflects a paradigm of proactive, sustained disease management rather than relying on a single, high-risk, potentially devastating surgical intervention.
C. Comparative Treatment Outcomes
The clinical evidence overwhelmingly favors the specialized endovascular approach for limb preservation and improved short-term safety profiles. The following comparative data synthesized from major clinical studies underscores the difference between traditional and modern intervention strategies.
Superior Outcomes: Endovascular Intervention vs. Open Surgery
Metric
Specialized Endovascular Intervention
Traditional Open Surgery (Bypass)
Impact on Patient Outcome
Risk of Amputation or Death
16% Decreased Risk (Risk-Adjusted)
Higher Baseline Risk
Maximally successful for life and limb preservation.
Complication Rate
Lower
Higher
Reduces post-operative morbidity and risk.
Hospital Stay
Shorter Duration
Longer, More Invasive Stay
Faster recovery and reduced risk exposure.
Early Mortality Rate (30-day)
Diminished Mortality (5.3% rate)
Higher Mortality (6.7% rate)
Demonstrates a superior safety profile in the immediate post-procedure critical window.
V. Meet the Specialist: Dr. Avishek Saha’s Comprehensive Toolkit for Advanced PAD
A patient seeking limb preservation requires assurance that their chosen physician is equipped not just for standard procedures, but for the complex, calcified, and potentially failed previous interventions that define advanced PAD. Dr. Avishek Saha’s practice focuses on utilizing the full arsenal of contemporary endovascular technology, ensuring preparedness for the most challenging arterial blockages.
A. Expertise in Complex Revascularization Techniques
Specialized peripheral intervention moves beyond conventional ballooning to address complex lesions, particularly Chronic Total Occlusions (CTO)—arteries that have been 100% blocked for an extended duration. Treating CTOs requires immense skill and specialized strategies, such as subintimal dissection and true lumen re-entry, which are frequently employed in complex revascularization scenarios. The presence of these highly technical skills signals an ability to manage cases often deemed “untreatable” by non-specialists.
The advanced services provided encompass a comprehensive range of state-of-the-art tools necessary for high technical and procedural success rates, even in the most difficult clinical scenarios. These advanced devices and treatments include:
Atherectomy: Mechanical removal of hard plaque buildup to prepare the vessel for ballooning and stenting. Although often used, registry data suggests careful selection for this approach.
Specialized Balloons: This includes conventional angioplasty (PTA), as well as Drug-Coated Balloons (DCB), which deliver medication directly to the vessel wall to prevent re-narrowing, and scoring or cutting balloons to facilitate opening rigid lesions.
Stenting Options: Both Drug-Eluting Stents (DES), which offer medication release to reduce recurrence, and standard Bare-Metal Stents (BMS) are utilized strategically, based on lesion morphology.
High technical and procedural success rates are achievable through the frequent and strategic use of these combination treatments. The ability to deploy atherectomy, specialized balloons, and navigate CTOs confirms the practice’s focus on limb salvage, reassuring patients—especially those with severe blockages—that they are consulting an expert prepared for the most intricate cases.
B. The Difference Between a Generalist and a Peripheral Intervention Expert
The difference between a generalist (like a primary care physician or sometimes a general cardiologist) and a specialized peripheral intervention expert is one of strategic focus. While a generalist focuses on risk factor management (medication, lifestyle changes), a peripheral intervention specialist, such as Dr. Saha, focuses acutely on restoring flow, preserving tissue, and achieving limb salvage.
The utilization of a vast and complex toolkit—including atherectomy, DCB, and techniques to manage severe CTOs—is the definitive evidence of specialized capability. It shows that the expert is capable of achieving revascularization in cases where generalized treatment may have plateaued or where a patient has received a poor prognosis elsewhere. Given that suboptimal implementation of existing evidence-based approaches contributes directly to the rising trend of non-traumatic amputations , seeking out a practitioner who consistently employs these advanced, successful strategies is the critical step toward avoiding irreversible damage. atypical heart attack symptoms kolkata
VI. Urgent Call to Action: Take Control Before the Damage is Done atypical heart attack symptoms kolkata
A. The Deadline: Why You Cannot Afford to Wait
The data presented here is not an academic discussion; it is a clinical warning. The stark fact that delayed intervention can increase the risk of a major amputation by nearly three times (Odds Ratio 2.96) should be treated as a definitive clinical deadline. Every day chronic leg pain is dismissed as “routine aging” is a day the underlying atherosclerotic plaque continues to build, pushing the patient closer to irreversible Critical Limb Ischemia (CLI). atypical heart attack symptoms kolkata
This immediate urgency aligns with broader public health objectives. Leading medical organizations, including the American Heart Association (AHA), have issued urgent calls for actionable policies to enhance the delivery of optimal PAD care with the goal of reducing non-traumatic lower-extremity amputations by 20% by 2030. A patient’s decision to immediately seek specialized assessment and intervention is a direct participation in this vital, limb-saving movement.
B. Secure Your Limb, Secure Your Future: Next Steps for Specialized Assessment atypical heart attack symptoms kolkata
If an individual experiences persistent chronic leg pain, cramping, non-healing sores, or if they possess known high-risk factors such as a history of diabetes (where PAD prevalence approaches 18% in the regional demographic ), high blood pressure, or established cardiovascular disease, an immediate specialized vascular assessment is mandatory. atypical heart attack symptoms kolkata
The most critical initial step is a comprehensive Peripheral Vascular Assessment, which must include routine Ankle-Brachial Index (ABI) screening, conducted and expertly interpreted by a peripheral intervention specialist. It is imperative that patients do not rely solely on a general diagnosis that fails to recognize the severity of systemic cardiovascular disease manifesting in the legs. Only specialized expertise designed explicitly for limb preservation and advanced revascularization can interrupt the dangerous pathway leading to amputation. atypical heart attack symptoms kolkata
C. Contact Dr. Avishek Saha Today
The path to proactive limb preservation and cardiovascular safety starts with one urgent, decisive action. Do not wait for symptoms to progress to the point of irreversible tissue damage or the threat of amputation.
Dr. Avishek Saha HealthcareContact Number: +91 9874381872 Website:www.dravisheksaha.com
Conclusion and Recommendations atypical heart attack symptoms kolkata
The evidence overwhelmingly establishes Peripheral Artery Disease as a widespread, escalating cardiovascular threat whose most devastating consequence, non-traumatic amputation, is often a direct result of delayed diagnosis and suboptimal care implementation. The high prevalence among regional high-risk groups, particularly diabetic patients, necessitates immediate and targeted screening.
The specialized approach of endovascular intervention, as practiced by experts like Dr. Saha, offers a statistically superior pathway for limb and life preservation, providing a risk-adjusted 16% reduction in amputation or death compared to traditional methods. The demonstrated capability to manage complex lesions, including CTOs and heavy use of advanced devices like atherectomy, confirms the practice’s focus on maximizing flow restoration where general treatment has failed. For any individual experiencing chronic leg pain or possessing known PAD risk factors, the recommended action is immediate consultation to leverage specialized diagnostics (ABI) and access advanced endovascular therapies before the disease progresses to critical, irreversible stages where the risk of major amputation increases nearly threefold.
I. Introduction to Cardiac Implantable Electronic Devices (CIEDs): The Foundation of Rhythm Management atypical heart attack symptoms kolkata
A. Defining the Clinical Spectrum and Scope of CIEDs atypical heart attack symptoms kolkata
Cardiac Implantable Electronic Devices (CIEDs) represent a crucial therapeutic class essential for managing a wide range of cardiac rhythm disorders. The clinical necessity for these devices spans from correcting profound bradycardia—characterized by a slow heart rate, disruption of electrical signals, and recurrent fainting spells—which is typically addressed by Permanent Pacemakers (PPMs) , to preventing sudden cardiac death (SCD) in high-risk patients via Implantable Cardioverter-Defibrillators (ICDs). atypical heart attack symptoms kolkata
The functionality of CIEDs defines a clear therapeutic hierarchy based on the required level of intervention. Standard PPMs focus on pacing support. ICDs provide both pacing and high-energy defibrillation capacity. At the apex of complexity are Cardiac Resynchronization Therapy devices (CRT-P, which provides pacing, or CRT-D, which includes defibrillation), which are designed to manage the mechanical inefficiency associated with advanced heart failure symptoms.
The successful outcome of CIED therapy is not merely predicated on the surgical execution, but on a strategic planning imperative. Implantation requires meticulous pre-procedural and intra-procedural decisions encompassing the selection of the appropriate device (single, dual, or triple chamber), determination of optimal venous access, precise lead positioning, and utilizing recommended connector types (such as the DF-4 connector). These strategic choices are foundational to long-term device function and the minimization of complications.
B. Key Contextual Factors in CIED Therapy
While the technical focus often resides on procedural success, an authoritative understanding of CIED therapy must acknowledge the patient’s lived experience. The commitment to CIED therapy is a long-term contract between the patient, the medical team, and the device manufacturer. Patients commonly express significant long-term concerns and fears, particularly regarding potential complications such as infection at the insertion site and the finite lifespan of the battery.
To provide truly expert guidance, the scope of care must address these fears practically. Success must be measured not only by immediate technical performance but also by the successful psychological integration of the device. Patients frequently experience body image disturbances and self-esteem issues due to the presence of a visible device, associated scars, and perceived limitations on physical activity. Comprehensive care, therefore, necessitates proactive interventions, including actively listening to and validating patient emotions, providing reassurance, and offering extensive patient education regarding device function and activity restrictions. Such robust support is essential for decreasing anxiety and preventing the immobilization that often accompanies high levels of fear. By linking the patient’s concerns directly to the technical risks analyzed in subsequent sections (e.g., minimizing infection rates and maximizing device longevity), the report establishes the critical human context that drives the pursuit of clinical excellence.
II. Technical and Clinical Complexity: Risk Stratification Based on Device Type atypical heart attack symptoms kolkata
The spectrum of CIEDs represents a continuum of procedural complexity, which directly translates into varying degrees of associated clinical risk. Analyzing these risks is crucial for assessing surgical quality and institutional protocols.
A. The Escalating Risk Profile of Advanced Devices
The complexity of an implantation procedure generally correlates with the number of leads required and the sophistication of the device’s function. A clear distinction exists between the risk profiles of simple and advanced systems. While transvenous ICDs remain the standard, there has been a notable movement toward non-transvenous alternatives, such as subcutaneous ICDs (S-ICDs) and extravascular ICDs, primarily because these options are associated with lower long-term complication rates stemming from the avoidance of intravascular leads. Furthermore, historical clinical preferences regarding device configuration have evolved; for instance, the historical preference for dual-chamber ICDs has largely shifted toward single-chamber ICDs to facilitate easier future extraction procedures.
B. Quantifying Morbidity in Cardiac Resynchronization Therapy (CRT) atypical heart attack symptoms kolkata
The implantation of Cardiac Resynchronization Therapy devices, which involve placing a third lead in the coronary sinus to pace the left ventricle, introduces the highest level of complexity. Data from large nationwide cohorts, such as a study involving 5,918 Danish patients who underwent CIED implantation, consistently confirm that patients receiving a CRT device (a triple-chamber system) exhibit the highest complication rate when compared with recipients of conventional single- or dual-chamber pacemakers or ICDs.
This heightened risk is not confined solely to de novo implantations. The decision to implant a triple-chamber device must be thoroughly considered, especially when compared with an alternative—waiting for a potential upgrade to CRT if the patient’s clinical status warrants it later. However, the procedure to upgrade an existing device to CRT is itself classified as a high-risk scenario. Follow-up data showed that CRT upgrades carry a significant 18.7% risk of any complication during the six months following the procedure.
This substantial risk associated with upgrades has a measurable clinical consequence, leading to therapeutic hesitation. The fear of complications related to an upgrade procedure can potentially prevent the transition to CRT, even in patients with clear clinical indications (e.g., Left Ventricular Ejection Fraction ≤ 30%, QRS duration ≥ 130 ms, NYHA Class I–IV symptoms). One retrospective study of ICD recipients found that 42.6% met the criteria for CRT at the initial implant, but the subsequent upgrade rate at five years was only 5.1%. This observed clinical inertia, driven by procedural risk perception, creates a significant gap between best-practice clinical indication and therapeutic implementation. This highlights that for complex devices, minimizing procedural risk is a prerequisite for ensuring patients receive appropriate, life-saving therapy when indicated.
C. The Impact of Patient Morbidity on Outcomes atypical heart attack symptoms kolkata
While surgical skill is a primary determinant of outcome, procedural complication rates are also profoundly influenced by underlying patient morbidity. In populations with specific anatomical and clinical challenges, such as patients with Adult Congenital Heart Disease (ACHD), the complication rates associated with ICD implantation are dramatically higher, ranging from 26% to 45%. These challenges stem from inherent anatomical complexities, the presence of intracardiac shunts, and limitations in vascular access to the ventricle.
This distinction necessitates that any comprehensive analysis of complication rates be carefully stratified. Standard complication data is clinically insufficient unless it differentiates based on device complexity (PPM versus CRT) and, crucially, patient complexity (general population versus specialized groups like ACHD). The presence of severe underlying patient morbidity may override even high levels of surgical expertise, underscoring the need for specialized centers equipped to handle complex anatomies.
III. Comprehensive Analysis of Procedural and Long-Term Complications atypical heart attack symptoms kolkata
Achieving optimal outcomes in CIED therapy requires minimizing immediate surgical risks, implementing robust infection control protocols, and providing comprehensive psychosocial support for long-term integration.
A. Minimizing Acute Procedural Risks atypical heart attack symptoms kolkata
Acute complications are those occurring immediately during or shortly after the implantation procedure. These surgical complications include pneumothorax, haemothorax, pericardial effusion, and pocket hematoma, all of which often necessitate further intervention.
A critical quality metric related to surgical finesse and technique is the rate of lead dislodgement. Data show that both atrial (1.22%) and ventricular (0.99%) lead dislocations are significant early complications. This risk is not randomly distributed but is strongly influenced by the volume and experience level of the implanting center, directly linking technical precision to institutional practice standards. The preferred technique for venous access, such as cephalic cutdown, over alternatives like axillary vein puncture, is part of a meticulous perioperative strategy aimed at reducing these acute risks.
B. The Persistent Threat of Infection: A Quality Control Indicator
Infection at the insertion site represents one of the most serious long-term complications. While surgical technique influences insertion site integrity, the epidemiology of CIED infection indicates that a large portion of this risk is controllable through rigorous adherence to protocol.
The omission of systemically administered prophylactic antibiotics during the first implantation has been confirmed as a significant risk factor for infection. Conversely, a meta-analysis established that preoperative administration of prophylactic antibiotics is effective in reducing the risk of infection, leading to a long-standing recommendation for their use before pacemaker implantation. Given this clear evidence base, a high incidence of infection rates in a center signals a failure in institutional protocol adherence rather than simply a technical surgical failure. Therefore, infection incidence functions as a critical metric for systemic quality control, demonstrating a center’s commitment to evidence-based preventive care.
C. Managing Psychological and Body Image Impact
The assessment of long-term complication management must extend beyond strictly physiological metrics to include the psychosocial impact. Patients often struggle with the psychological presence of the device, leading to body image disturbances and self-esteem issues. The physical evidence of the device and associated scars, along with limitations on certain physical activities, can lead to feelings of self-consciousness and fear of societal judgment.
High-quality centers integrate this awareness into their care model. Interventions include comprehensive patient education—ensuring the patient and family understand the device function and necessary activity restrictions—and providing active emotional support. True care quality requires integrating technical precision (low dislodgement) and protocol adherence (low infection) with robust psychosocial support. By actively validating the patient’s concerns and providing knowledge, the healthcare team can decrease the fear that might otherwise lead to prolonged immobilization and impaired quality of life.
IV. Device Integrity, Longevity, and Safety Alerts: A Deep Dive into Non-Procedural Risks
Beyond the immediate risks of surgery, patients face risks inherent to the long-term function of the electronic device itself. These non-procedural risks are independent of the surgeon’s skill but demand specialized clinical vigilance for monitoring and management.
A. The Challenge of High Battery Impedance
A notable and critical area of non-procedural risk involves issues related to device battery integrity, specifically the phenomenon of high battery impedance. Recent safety advisories have targeted specific subpopulations of pacemakers and CRT-Ps manufactured by Boston Scientific (e.g., ACCOLADE, PROPONENT, ESSENTIO, ALTRUA, VISIONIST, and VALITUDE lines built before September 2018). The underlying mechanical cause for this high impedance varies by device line but generally relates to latent manufacturing flaws: either higher concentrations of lithium salts in the battery cathode or insufficient electrolyte from latent absorption.
This high internal battery impedance is problematic because it causes the available voltage to drop during periods of high battery consumption, such as remote telemetry interrogation or other normal, higher-power operations. The failure mechanism is not simply the battery reaching its end-of-life projection, but rather a sudden system failure triggered by a high-power demand event.
The consequence of this sudden voltage drop is a system reset. Multiple consecutive resets within a short period (e.g., three resets in 48 hours for the INGENIO line) can force the device into a non-programmable Safety Mode. This Safety Mode is designed as a fail-safe, but paradoxically, it introduces severe clinical risk. The fixed, non-programmable settings—such as VVI pacing at 72.5 beats per minute at 5.0 V and 1.0 ms output—may not provide optimal cardiac support for the patient’s underlying condition.
The results of safety mode operation can be catastrophic, particularly for pacemaker-dependent patients. Clinical harm reports include pacing inhibition or pauses, loss of atrioventricular synchrony, heart failure decompensation, and muscle stimulation (e.g., skeletal muscle or phrenic nerve stimulation) from the high output. Most severely, the worst-case reported patient harm has involved loss of pacing, leading to serious injury or life-threatening outcomes, including two reported deaths in pacemaker-dependent patients.
The prevalence of this specific failure mode increases dramatically over time, demanding specialized monitoring. Postmarket surveillance data shows that the prevalence of safety mode backup pacing due to high impedance can range significantly, reaching up to 49% at 11 years for some device lines. This escalating risk requires that ongoing follow-up care must move beyond simplistic projected battery life; clinical teams must actively monitor impedance trends, especially before conducting high-power procedures like device interrogation or telemetry.
The repeated necessity for advisories regarding different device lines linked to different manufacturing flaws (lithium salts versus electrolyte levels) strongly indicates a systemic quality control challenge within the industry that demands robust post-market surveillance.
Table 4: Analysis of Boston Scientific CIED Device Advisory Risks (Manufacturer-Related Failures)
V. The Volume-Outcome Nexus: Quantifying Quality Metrics in CIED Implantation
The relationship between the frequency of a procedure (volume) and the resultant clinical success (outcome) is a fundamental metric in healthcare quality assessment. For CIED implantation, this relationship provides an evidence-based framework for selecting high-quality providers.
A. Establishing the Volume-Outcome Relationship
Extensive research across various cardiothoracic procedures, including coronary artery bypass grafting, consistently shows that hospitals and surgeons who perform a higher volume of procedures achieve lower mortality and complication rates compared to those with lower volumes. This inverse relationship is so significant that procedural volume thresholds are commonly incorporated into accreditation standards and quality metrics by regulatory and professional organizations. For cardioverter-defibrillator implantation specifically, several studies have demonstrated this inverse correlation between institutional volume and complication rates.
B. Statistical Validation and the Critical Volume Threshold
To empirically test this association in Permanent Pacemaker (PPM) implantation, a retrospective examination of data from the German obligatory quality assurance program was conducted, involving 430,416 PPM implantations across 1,226 hospitals. This analysis demonstrated a clear and significant correlation: as the hospital annual PPM volume increased, there was a corresponding decrease in procedural and fluoroscopy times, as well as reduced rates of early surgical complications and lead dislocations (P for trend <0.0001).
Crucially, this study identified a statistically validated threshold for high risk. The greatest disparity in outcomes was observed between the lowest volume quintile (1–50 implantations/year) and the second-lowest quintile (51–90 implantations/year). Hospitals that successfully moved out of the lowest volume group achieved significantly reduced risks: the Odds Ratio (OR) for surgical complications dropped to 0.69 (95% CI 0.60–0.78), and lead dislocations (atrial and ventricular) were also significantly lower (ORs between 0.69 and 0.73).
The volume threshold of less than 50 PPM implants annually is thus confirmed as a statistically validated zone of high institutional risk. High-volume centers successfully mitigate complexity; despite performing a relatively higher percentage of complex devices (e.g., dual chamber, CRT), they maintain lower complication rates, confirming that expertise derived from volume successfully overrides the inherent risks of complex systems. This provides a clear, actionable data point for institutional strategy and provider selection.
Table 2: Influence of Hospital Annual Volume on Pacemaker Implantation Outcomes (Based on German Registry Data)
Annual Hospital PPM Volume Quintile
Relative Procedural Time/Fluoroscopy
Risk-Adjusted Surgical Complications (Composite)
Odds Ratio (OR) for Surgical Complication (Lowest Quintile Reference)
Lead Dislocation Risk (Atrial/Ventricular)
Lowest (1–50)
Highest
Highest
1.00 (Reference)
Highest
Second Lowest (51–90)
Decreased
Significantly Lower
0.69 (CI 0.60–0.78)
Lower (OR 0.69 – 0.73)
Highest Quintiles
Lowest
Lowest
Significant P for trend <0.0001
Lowest
C. Systemic Expertise and Staff Proficiency
High procedural volume must be understood as a metric not just for the lead operator, but for the proficiency of the entire surgical support structure. Optimal outcomes are dependent on the presence of centers with high-volume operators (as centers with <50 implants/year have demonstrated higher complication rates) and, importantly, at least one dedicated, non-scrubbed nurse or allied professional who is proficient in supporting complex device procedures. This necessity confirms that superior quality is a systemic achievement, relying on consistent team familiarity and expertise.
While volume is established as a critical metric, ongoing inquiry is necessary to fully determine if the volume-outcome relationship applies uniformly across a surgeon’s career arc, distinguishing between junior surgeons (in the first five years post-training) and established surgeons (in practice for over five years).
VI. Global Standards and Centers of Excellence: Evaluating Expertise and Access to Care atypical heart attack symptoms kolkata
The pursuit of excellence in CIED implantation is increasingly a global endeavor, with several regions establishing world-class quality benchmarks, often challenging traditional notions about the correlation between cost and care quality.
A. International Accreditation and Quality Benchmarking
Global quality in cardiac device implantation is standardized through adherence to internationally recognized accreditation bodies, such as the Joint Commission International (JCI), National Accreditation Board for Hospitals & Healthcare Providers (NABH), and National Accreditation Board for Testing and Calibration Laboratories (NABL). These bodies guarantee globally benchmarked care and safety standards, ensuring consistency regardless of the operating region. High-volume, complex cardiac procedures are measured by their success rates, with benchmarks exceeding 90% to 98% demonstrating effective management of complex cases.
B. The Rise of Global High-Volume Centers (Case Study: India)
India has emerged as a significant global leader in cardiac pacemaker implantation. This status has been achieved by providing life-saving procedures at a significantly reduced cost compared to Western nations while robustly maintaining high standards of quality. With a nationwide average success rate for pacemaker surgeries exceeding 90%–98%, the country attracts patients from over 140 nations.
Leading institutions, such as Fortis Escorts Heart Institute, report elite heart rhythm center success rates often above 98%. Similarly, Apollo Heart Institutes, recognized globally and ranked among top hospitals by publications like Newsweek, reports success rates exceeding 95% in complex cardiac surgeries, establishing them as international referral centers for pacemaker implants. This high standard of efficacy is replicated in more complex procedures, with AICD (Automatic Implantable Cardioverter-Defibrillator) implantation success rates also typically exceeding 90%. The fact that these verified high success rates exist alongside international accreditation demonstrates that achieving a high standard of quality is decoupled from high cost when appropriate infrastructure and high procedural volumes are concentrated. Furthermore, centers like Manipal Hospitals demonstrate a commitment to technological leadership through the adoption of innovations such as AI-powered leadless pacemakers and robotic assistance.
VII. Case Study in Regional High-Volume Expertise: Interventional Cardiology in Kolkata atypical heart attack symptoms kolkata
The abstract principle of the volume-outcome relationship must be validated by concrete examples of individual expertise. A high-volume specialist operating within an accredited system serves as the archetype for quality care.
A. Profile of a Comprehensive High-Volume Specialist
Dr. Avishek Saha in Kolkata exemplifies an interventional cardiologist whose practice aligns with the high-volume standards established by clinical research. His expertise is expansive, covering the full spectrum of rhythm management, including Pacemaker, ICD, and CRT implantation, alongside complex coronary interventions such as Coronary Angiography and Angioplasty (PCI), as well as structural heart interventions like device closures for ASD, VSD, and PDA. This combined high volume across interventional disciplines suggests a synergistic skill set where precision required for complex stenting translates directly to the technical demands of challenging venous access and lead placement necessary for advanced CIEDs like CRT devices.
B. Verifying High Procedural Volume
The critical validation of quality lies in verifiable procedural numbers. Dr. Saha has independently performed more than 500 Pacemaker Implantations. This figure significantly exceeds the statistical institutional high-risk threshold of <50 implants annually. Furthermore, his experience includes over 1,500 Coronary Angioplasties. These documented numbers provide a robust performance metric, validating the abstract volume-outcome research with concrete, individual performance data, thereby serving as a definitive trust metric for patients and institutions alike.
C. Infrastructure and Integrated Care
A critical factor enabling consistent high-quality care is institutional affiliation. The specialist maintains affiliations with multiple trusted, high-standard institutions in Kolkata, including Manipal Hospitals and Fortis Hospital. This ensures that the specialist consistently has access to cutting-edge cardiac technology and high-quality infrastructure required for successful outcomes in complex cases. By offering a comprehensive suite of cardiovascular services, including advanced device implantations, under one specialist or clinic, the care delivery is streamlined. This integrated approach ensures continuity and efficiency for patients who often require multifaceted cardiac management.
Table 3: High-Volume CIED Expertise and Quality Benchmarks
Quality Metric
Target Threshold (Individual/Institutional)
Significance
Example
Source
Institutional Annual Volume
≥ 51 procedures/year
Avoids highest institutional risk quintile (OR 0.69 for complications)
Benchmark for high-quality outcomes across device types
Leading accredited hospitals in India (Apollo, Fortis)
Systemic Quality Control
Mandatory Protocol Adherence
Minimizes preventable risks, e.g., using prophylactic antibiotics
Evidence-based care requirement
VIII. Strategic Recommendations for Patient Selection and Provider Due Diligence
A. Framework for Patient Decision-Making
Patients facing CIED implantation must engage in rigorous due diligence based on quantitative risk assessment. They must first understand that their specific complication risk is tied directly to the complexity of the prescribed device (PPM versus the inherently riskier CRT) and their unique medical profile (e.g., the significantly elevated risk associated with ACHD status).
In vetting providers, patients should prioritize centers that demonstrably operate above the statistical risk threshold, ideally those with an annual volume of at least 51 implants. Furthermore, prioritizing specialists with verified, high individual volumes, such as those documenting 500 or more procedures, ensures access to the highest level of acquired expertise. Finally, prospective patients must engage in comprehensive psychological preparation, leveraging available patient education and emotional support resources to proactively mitigate long-term fears regarding device function, infection, and body image integration.
B. Recommendations for Institutional Quality Improvement
Institutional efforts to optimize CIED outcomes must focus on systemic controls and verifiable performance metrics:
Standardize Infection Control: Institutions must establish and strictly enforce protocols mandating the systemic administration of prophylactic antibiotics before all primary implantations to eliminate this critical, preventable risk factor.
Ensure Team Proficiency: Beyond the lead operator’s skill, investment must be made in training and retaining allied healthcare professionals. The presence of a non-scrubbed nurse or technologist proficient in device support procedures is critical for achieving lower systemic complication rates.
Mandatory Meticulous Planning: Detailed, written perioperative plans must be required for all complex CIED implantations (ICD, CRT, and upgrades). This proactive planning is essential to address complexities related to access, lead management, and managing potential antithrombotic regimens.
C. Conclusion: Defining Excellence in Cardiac Rhythm Management
Excellence in Cardiac Implantable Electronic Device therapy is a comprehensive outcome, defined by the successful convergence of multiple quality domains. It demands an evidence-based procedural strategy that carefully navigates the escalating risk associated with device complexity. It relies on demonstrated high volume expertise, validated by quantitative procedural metrics, to minimize acute surgical complications like lead dislodgement and pocket hematoma. It requires rigorous protocol adherence, particularly concerning prophylactic antibiotics, to mitigate preventable infection risk. Finally, excellence necessitates proactive, sophisticated technical surveillance to monitor for long-term device integrity issues, such as the potentially lethal cascade failure triggered by high battery impedance during routine telemetry. Only through this multi-faceted approach can patient safety be maximized and long-term quality of life be guaranteed.
Every year, thousands of brilliant students from Kolkata and districts like Howrah, Hooghly, and Bardhaman start their journey towards the West Bengal Civil Service (WBCS). They have the dedication, they buy the right books, and they study for 10+ hours a day. common mistakes WBCS aspirants
Yet, when the results come out, many are shocked to find their names missing from the list. common mistakes WBCS aspirants
Why?
It’s rarely a lack of hard work. Usually, it is a lack of direction. After mentoring hundreds of successful officers at Trademark IAS, we have identified 5 “Silent Mistakes” that quietly destroy a candidate’s chances before they even sit for the exam.
Are you making any of these? Let’s find out.
1. The “College Street” Collector Trap common mistakes WBCS aspirants
Kolkata has a blessing that can also be a curse: College Street. A common mistake beginners make is visiting Boi Para and buying every recommended book in the market. You have Laxmikanth for Polity, Spectrum for History, plus 3 other “suggested” books for the same subject.
The Reality: You end up with a library, not a strategy. Buying more books leads to “Resource Overload.” You read five books once, instead of reading one good book five times.
The Fix: Stick to the One Subject = One Source rule. For WBCS, mastering the basics (NCERTs + Standard Texts) is far more important than reading advanced research papers.
2. The “Prelims Phobia” (Ignoring Mains) common mistakes WBCS aspirants
This is the single biggest reason for failure. Many aspirants spend 90% of their year preparing only for the WBCS Prelims. They think, “Let me clear Prelims first, then I will study for Mains.”
The Reality: The gap between Prelims and Mains is often just 3-4 months. That is not enough time to cover the vast Mains syllabus, Optional Subject, and Language papers. If you study only for Prelims, you might clear it, but you will likely crash in the Mains.
The Fix: Adopt an “Integrated Strategy.” Prepare for Mains from Day 1. Since the syllabus overlaps by 70%, your Mains preparation will automatically help you clear Prelims with a high margin.
3. Paralyzed by “Syllabus Anxiety” (Old vs. New Pattern) common mistakes WBCS aspirants
With recent news about the WBPSC potentially changing the WBCS syllabus to match the UPSC pattern, many students are paralyzed. They spend hours watching YouTube videos speculating on “Will 2026 be descriptive?” instead of studying.
The Reality: History, Geography, Polity, and Economy do not change. Whether the exam is MCQ (Objective) or Written (Descriptive), the core content remains the same. The Constitution of India won’t change just because the exam pattern does.
The Fix: Stop speculating. Focus on building core concepts. If you understand the “Why” and “How” of a topic (UPSC style), you can answer both MCQs and written questions easily. At Trademark IAS, we teach concept-first to “future-proof” our students.
4. The “PDF Collector” Syndrome
In the age of Telegram channels, students hoard thousands of PDFs—current affairs, topper notes, summaries. They download them, save them in a folder labeled “Read Later,” and never look at them again.
The Reality: Digital hoarding gives you a false sense of accomplishment. You feel like you are studying, but you are just organizing files.
The Fix: Limit your digital diet. Follow one reliable daily news analysis and one monthly magazine. Make your own handwritten notes. The act of writing helps your brain retain information 3x better than reading a PDF.
5. Isolation: The “Lone Wolf” Mistake
Many aspirants lock themselves in their rooms, cut off all social contact, and try to fight this battle alone. They believe coaching is a waste of money and self-study is enough.
The Reality: While self-study is crucial, isolation is dangerous. Without a mentor or a peer group, you have no one to correct your mistakes, no one to evaluate your answers, and no one to pick you up when you feel demotivated.
The Fix: You don’t need a factory-style coaching center with 500 students. You need Mentorship. At Trademark IAS, we follow a “Gurukul” approach with small batch sizes. We don’t just teach; we evaluate your progress weekly, correct your answer writing, and keep you on the right track.
Stop Making These Mistakes Today
Success in WBCS or UPSC is not about who is the smartest; it is about who makes the fewest mistakes.
If you recognized yourself in any of these points, don’t panic. Recognizing the problem is the first step to fixing it.
Need a personalized strategyto fix your preparation? Come visit us at Trademark IAS in Kolkata. Let’s build a roadmap that works for you.